Colorectal Cancer
Can Be Prevented
What Can I Do?

The best thing you can do to prevent Colorectal Cancer is to screen for and remove any polyps. |
Colon cancer is unique because it can be almost completely prevented through screening. Other cancers, such as breast or prostate cancer, can be detected early through screening, but not before the cancer has already developed. Since colorectal cancer usually develops from non-cancerous (benign) polyps in the colon, finding and removing these polyps can actually prevent cancer from forming.
By age 50, at least one in five people has polyps. Most people have an excellent chance of preventing colorectal cancer by regular screenings to find and remove polyps before cancer develops. Detecting such polyps and other colon abnormalities requires an effective screening procedure by a qualified physician.
Possible Screening Methods are:
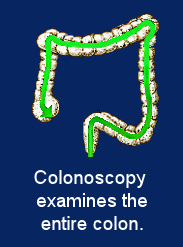
- Colonoscopy: Considered the gold-standard in colorectal cancer screening, it is the only method to lower colon cancer deaths by removing polyps during the screening.
Colonoscopy is the only technique to provide a direct, close-up view of the inside of the entire colon. A long, narrow, flexible tube containing a fiberoptic camera and lighting is inserted through the rectum and carefully advanced to the end of the colon (the cecum, where the colon joins the small intestine).
The doctor observes your colon directly through the scope or enlarged on a television monitor. Photos and/or videos can be kept with your medical chart for later reexamination.
During your test, your doctor usually removes any polyps using a wire loop, sealing the tiny cut with a mild electrical current. Polyps, found in at least 20% of patients, are tested at a lab for cancer cells.
Use a board-certified gastroenterologist well-trained and experienced
in colonoscopy. These doctors have the detailed knowledge of the digestive system to best interpret findings. |
Colonoscopy is performed by specially-trained physicians called endoscopists. While most are gastroenterologists, a few surgeons and even some general internists have had endoscopy training.
The American Cancer Society recommends a screening colonoscopy at least once every ten years from age fifty; sooner if you have a family history of colorectal cancer or polyps. Patients prepare with a colon cleansing routine.
 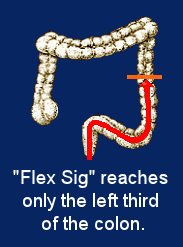
- Flexible Sigmoidoscopy: This method also uses fiberoptics but only reaches one-third of the colon. Polyps or abnormalities in the other two-thirds cannot be found and removed. Less than forty percent of polyps are found by this method, leaving unseen polyps which may continue developing toward cancer. Some groups of people, including African Americans, have an even higher percentage of polyps found in the right colon. Therefore, most knowledgeable physicians are reluctant to use this test for screening.
Although the American Cancer Society lists this as a screening option when done every five years with an annual Fecal Occult Blood Test, this combination is not nearly as effective as colonoscopy, which visualizes the entire colon. Use “flex sig” only when reliable colonoscopy is not available
to you.
- Fecal Occult Blood Test (FOBT):
This involves collecting one or more samples from bowel movements and sending them to be tested for the presence of any occult (hidden) blood.
Damaged blood vessels on the colon wall or the surface of polyps may bleed. That’s why blood in stool is a symptom of cancer or pre-cancerous polyps. Alert your gastroenterologist immediately if you see such blood.
Bleeding, however, is often not visible to the eye. An FOBT analyzes stool for microscopic traces of blood. If blood is found, a colonoscopy is required to find its source. The cause might be as insignificant as a hemorrhoid, or as serious as full-blown cancer.
Results showing no blood do not prove anything since polyps or abnormalities may simply not have bled at the time of the sample. Several stool samples taken at different times increase the chance of finding blood, but not all polyps, or even cancers, bleed more than healthy tissue.
| Bottom line: With FOBT, if you find blood you must get a colonoscopy. If you don’t find blood, you’re still not assured a clean bill of colorectal health. |
As with flex sig, we recommend FOBT only if colonoscopy is not available. FOBT is probably better than nothing. If you must use FOBT for any reason, insist on the multiple sample system. |
- Double Contrast Barium Enema (DCBE): This test allows a doctor to analyze the colon using X-rays. It’s rarely used today for colorectal cancer screening. DCBE has never been rigorously tested to prove its effectiveness as colonoscopy has.
Since traditional X-rays pass through the colon without producing any images, radiology staff must fill the colon with liquid barium, given as an enema, to reflect x-rays and provide images. Patients must clean out the colon with laxatives and a regular enema beforehand.
Once the colon is filled with the barium, air is also pumped in to inflate the colon further, like a balloon, before the x-ray is taken. The patient must hold the air and liquid barium in the bowel during radiography. This causes cramping and an urgency to empty the bowel. Sedation is not usually offered.
- Virtual Colonoscopy: Click Here for information on "Virtual Colonoscopy"
Page 4
|






